I’m back with another Public Service Announcement personal-experience post, because when I manage to run afoul of some innocuous thing, such as a door, I feel morally obligated to share. You can learn from my follies and foibles. At any rate, it’s good to maintain a level of wariness when it comes to hidden dangers in your own environments.
In case you missed them, here’s:
the time I almost amputated my foot with a steel security screen door,
the result of my subsequent failure to go to the E.R. for stitches, and
the time I walked off a loading dock without realizing that it was a loading dock.
(I also wrote about the time I tripped and fell on the sidewalk, but that’s not weird. Everyone trips and falls on sidewalks at some point.)
Anyway, if you’re curious about this latest fiasco, fix yourself a drink or a cuppa and settle back to read my tale of woe. Some of you… maybe especially you who’ve known me the longest… are going to laugh, or eye-roll, or facepalm, or all of the above, and I’m okay with that. I’m right there with you. I believe I’ve outdone myself this time, friends.

Yeah. Really. [25 May 2023]
At 10:15pm Wednesday, May 10, I took a vitamin, the same one I take every night… only this time, instead of going down my esophagus into my stomach, the vitamin went down my trachea into my lungs.
And now I have multifocal aspiration pneumonia. Yeah. I have pneumonia as a consequence of taking a vitamin.
Right?!
Aspirating that vitamin took considerable talent, my friends. It was a horse pill. I’m not even sure how I did it. Of the various mishaps I’ve experienced over my lifetime, one of them has to be the weirdest, and this is it… the weirdest of my weird mishaps.
If you’re wondering what it felt like in the aftermath, imagine someone setting fire to your lungs. I’m trying to think of another time I’d characterize pain as “burning,” and I can’t recall a burning pain instance that could rival this one. It was ghastly.
At the E.R., I was examined and reassured that I wasn’t going to die. I was skittish when the Lidocaine appeared before me in a little paper cup. It would numb my throat, they warned, and that made me nervous. I declined. I went home. But the pain worsened until I had no choice but to go back to the E.R. – it was 3:00am, and I was in agony. I went in with my proverbial tail between my legs and begged for the damn Lidocaine cocktail.
I expected the Lidocaine to taste vile, but the reality is that nothing is truly vile if it extinguishes fire in your lungs and throat. It was thicker than the thickest paint, and it tasted like paint, too, but the relief was immediate. It cooled the inferno in my chest cavity.
We got home just after 5:00am. I called in to work, fell asleep, and woke up at 11:00am with an intense headache and a fever of 100.6. But the pain in my lungs and windpipe was gone!
My fever fluctuated all day, up and down. The next morning I felt like I should go to work, so I did. I thought that that was the end of it. I thought that the crisis was over. When a nurse called from my primary care physician’s office, though, she said that because of my fever, I should go back to the E.R. to get checked out.
The next day was Saturday. I felt worse… coughing, wheezing, feverish. Short of breath. Exhausted. At the E.R., I was diagnosed with aspiration pneumonia, which you can get when a foreign object invades your lungs. Of course.
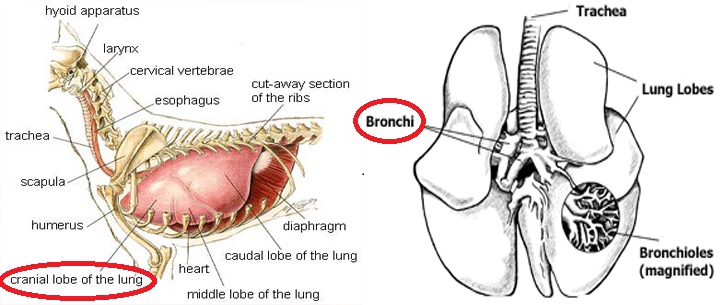
There commenced, over the next two weeks, several daytime stays at the hospital. I.V. antibiotics. I.V. fluids for hydration. Breathing treatments. Numerous vials of blood for testing, several chest X-rays, two contrast C.T. scans, and even an E.K.G., for some reason. At some point, the word “multifocal” was added to my diagnosis, because they found pneumonia in two different parts of my lung (both the middle and the lower right lobe). The doctors – my primary care physician and pulmonary specialist – extended my course of antibiotics, and also put me on Prednisone (steroids).
Be patient with your recovery, they cautioned, because multifocal pneumonia is generally more severe than pneumonia that affects only one part of the lung lobe. (This has already been my experience. The first and only other bout of pneumonia I had – back in 2020 – involved just one part of my lung, and this time is definitely worse.)
Two days ago, I went back to work after two weeks out. I’m still wheezing, wet coughing in the morning and dry coughing during the day, short of breath and using the Albuterol inhaler. But my blood oxygen levels are great, and all of my other symptoms are gone (for the most part).
I’m well on my way out of this mess, but it’s going to take a while for my lung to return to normal. I’ve been warned that relapse can occur and the pneumonia can come back full-force if I overdo it before full recovery, so I have to resume my normal activities slowly. Lightly. I felt worse when I woke up yesterday morning; it wasn’t the best idea to do a full 8-hour workday my first day back. I should’ve started with a half-day. Somehow, that didn’t cross my mind.
It’s just hard to remember that while the acute phase is over, I’ve not yet recovered. Full recovery from multifocal pneumonia will take three to six months. I have to keep reminding myself of this. (The first time I had pneumonia, it wasn’t multifocal, and it took five months for my chest X-ray to clear).
I have to be mindful of my physical limitations, which is hard, as I like to be active and do things. I can’t move quickly, can’t lift. I need to continue “taking it easy” until I’m fully recovered, because to do otherwise would be risking relapse.
As for my 2023 fitness journey? HA HA HA! This is what I was talking about when I said it was “start and stop” in my last post. I can’t work out again until I get exercise clearance from my doctor, and when I do, I have to keep the duration and intensity level of the workouts to 50% at the most… and I won’t be able to get that clearance until I see my primary care physician in two weeks.
So this is the PSA part:
–Don’t aspirate foreign objects into your lungs.
–If you do, take the Lidocaine cocktail when they give it to you at the E.R.
–If you develop a fever following the incident, do not go to work the next day! GO TO THE E.R. ASAP.
–When you do go back to work, don’t jump in with a full day. Start with a half-day. When the doctors say “ease back into it,” do.
And that’s the story of the last few weeks. Of my latest ridiculous freak accident. I have upcoming appointments with Primary Care and Pulmonary as they monitor my progress. I’m happy that I can sleep lying down now (I couldn’t before, because lying down caused coughing fits), I can speak full sentences without running out of breath, I can taste things again, and I have an appetite. At the beginning of the pneumonia, all I wanted to eat was fresh watermelon, pineapple, and popcorn. I still crave those things and eat them every day – I am blessed – but now I’m able to eat other foods.
I can’t say enough how much I appreciate the doctors, nurses, technicians, and staff at the Phoenix V.A. The Phoenix V.A. takes a beating in the media, and it’s undeserved. The health care I receive there is wonderful!
Blessed.
Be careful out there, friends.